Please register to participate in our discussions with 2 million other members - it's free and quick! Some forums can only be seen by registered members. After you create your account, you'll be able to customize options and access all our 15,000 new posts/day with fewer ads.
Single payer to cover a standard level of care for all citizens, including basic preventive services, hospitalization, maternity, etc, or what I call "medicare for all". We're a rich country, we have the technology, it's time. Higher levels of supplemental coverage available on the individual market. No employer based coverage. Done.
That won't work and we know it. There is simply not enough money, period. Let's do some math.
The total amount of money spent on healthcare in the U.S. in 2011 was $2.701T according to a recent JAMA article (Moses et al. "The Anatomy of Health Care in the United States," JAMA 2103; 310(98): 1947-1963. Go read this article. It is a great wealth of information even though the commentary is predictably left-wing as it is JAMA. It does not have any of the extrapolations I did below, which I really wish they would have done as an academic exercise.) Note that the figures are from 2011 and those expenditure numbers are all pre-Obamacare and thus include a lot of people with no insurance not drawing on the system and also people with less-expensive "substandard" insurance. But just for this exercise, we'll use that number. The entire revenue of the federal government that year was only $2.303T according to the CBO. We would need to increase federal revenues 18% just to pay for the "substandard" healthcare in 2011 for the number of people who had insurance in 2011. Assuming this would replace Medicare/Medicaid, we'd still have another $2.763T in federal expenditures to fund the rest of the government. Total federal expenditures would be $5.464T, or 237% of total federal revenues and 48% of that year's private sector GDP ($11.393T). You would have to take half of every dollar made in the private sector just to fund healthcare that Obama called "substandard" and that doesn't even cover the ~15% who had no health insurance in 2011.
Okay, so you say there are people on "Cadillac plans" driving up the cost of health care and you actually want to have "Medicare for all." Let's run those numbers. Medicare covered 11% of people in 2011 (34.2M people) and was responsible for 20.5% of total expenditures ($554B.) Medicare's expenditures per beneficiary are thus $16199. Extending that to the entire population of 311.1M would cost $5.04T just for Medicare. Total federal expenditures would be a whopping $7.803T! To be accurate, that figure is a massive overestimation as Medicare mainly covers the over-65 set which do have a higher proportional cost. The over-65 set in 2010 was ~13% of the population and accounted for 34% of total health spending. So if we weight the Medicare figures for the under-65 population by their relative percentage of expenditures (66% of spending for 87% of the population), we get a per-under-65-person spending of $6188. That would make the total "Medicare for All" spending approximately $2.33T. That figure is pretty darned close to the total healthcare expenditures in the country in 2011 of $2.701T and would require again pretty close to seizure of half of all of the privately-made goods and services in the United States to pay for it and the rest of the government's spending at 2011 levels.
However there is another problem with "Medicare for All." Medicare only reimburses hospitals and docs at about 85% of the cost required to provide care. The hospitals absolutely depend on having enough privately insured patients to make up this difference as commercial insurers pay about 130% of the cost of providing care. Medicaid pays even less than Medicare and as a result very few places take Medicaid patients. "Medicaid for All" would result in the same situation with Medicare as hospitals and docs would close up rather than take a 15% loss on everybody they see. So you'd have insurance that nobody takes or you would have to reimburse at a higher rate so that hospitals and doctors can at least break even and have some money left over for things like maintenance, replacing old equipment, expansion, and paying for necessary ancillary staff. Obama says a 15% total overhead is OK for insurers, so let's use that for reimbursements- 115% of the cost of providing direct care. That would require a whopping 35% increase in Medicare costs and the total amount spent on "Medicare for All" would be $3.15T. We'd see 52% of the private sector GDP seized to pay for this and the rest of the 2011 levels of federal expenditures ($5.91T.)
There, you should see that the math simply does not work out. The only way to attempt to make any sort of universal healthcare work out is to severely ration it. We already are running unsustainable budget deficits with the current ~$835B in federal Medicare/Medicaid spending, let alone 3-4 times that much as in a hypothetical "Medicare for All" scheme. You'd have some very, very severe rationing such as the UK NHS's recently-changed "nobody over 50 goes to the ICU, ever" rule. That would not be terrifically useful either.
Where would the new competitors come from without getting bought up?
As long as an insurance company stays in-state, the FTC has no say. The states can take action (since most states have anti-trust laws), but they could take action today and choose not to. That is why even if you remove the state by state restriction, BCBS, Cigna, Coventry, etc can keep their "federation" format and avoid any anti-trust actions.
The issue is currently that another company from another state can't come in and offer policies. Also, the FTC should have jurisdiction as a multi-state association of statewide insurers such as the BCBS Association certainly IS interstate commerce and thus the FTC can have jurisdiction. Shoot, a farmer growing about $800 in today's dollars worth of wheat for his personal use and had that declared "interstate commerce" in Wickard v. Filburn. Multibillion-dollar insurance company trusts should certainly fall under that jurisdiction if half a combine load of wheat that never left a farm did.
Quote:
Originally Posted by marigolds6
Texas implemented this system over a decade ago.
10 years later,
Number of lawsuits dropped from ~1275 to ~450. Average payout from ~$225,765 to $198,673.
Aggregate payout dropped from $225M to $48M statewide. But malpractice underwriters left the state in big numbers, so after an initial drop in malpractice premiums, aggregate premiums climbed back up to original levels and there was no net savings to practitioners as a group. But, the number of practitioners increased in urban areas (decreased in rural areas), so premiums to individual practitioners dropped. Though aggregate premiums are the important number here, since that is the amount of premiums ultimately passed on to health care consumers in the state.
You forget that there happened to be a ~20% population growth rate in Texas during that time period. The aggregate amount spent on premiums being the same post-tort-reform but with 20% more people is a big deal as each person in the state has 20% less in malpractice insurance premiums passed onto them. You are trying to make it sound like this was a failure but it is not. Again, do the math.
Quote:
Meanwhile, post-surgical disability claims jumped dramatically, reflecting a real possibility that the drop in malpractice claims was absorbed by the public through welfare grants. Essentially tort reform become a huge subsidy to insurance underwriters and a mild subsidy to the medical industry, paid for by taxpayers while health care consumers saw no decrease in costs (the increase in practitioners also oddly did not reduce health care costs in the state).
Disability claims nationwide have jumped precipitously in the past five years nationwide. It's not just a Texas thing. The main reasons cited by CNN of all places are that people are mainly using it as a form of welfare due to the poor economy and actual welfare being harder to get onto than it was before the 1990s. It has nothing to do with subsidizing insurance companies.
Also, of course you won't see a decrease in total medical costs in a state when you have a 20% population growth! You have 20% more people to take care of. Again, do the math.
Only if we replace it with something resembling the insurance systems in the rest of the west. Otherwise, no.
Why are you so anxious to end the ACA now, well before it has been fully enacted and had an opportunity to produce meaningful and measurable results?
Are you that afraid that despite its early implementation issues it will be a success?
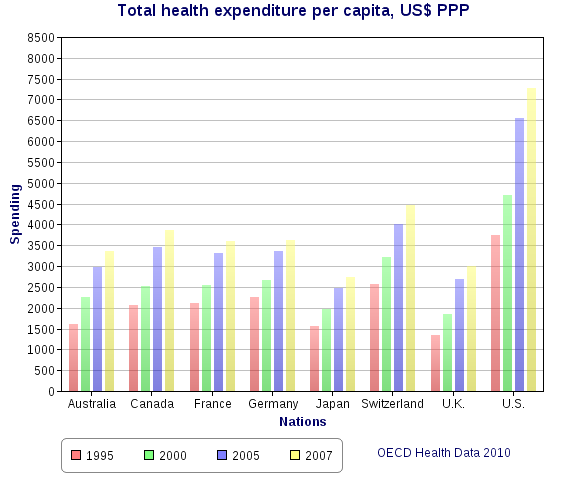
And what do you have to say about the discrepancy between what we pay and get and what Canadians (only 0.5% of whom cross our border for care, typically because they are traveling), Japanese, much of Europe, pay and get?
Why is the right so full of whiners?
It should be ended before the employer mandate kicks in, which will force many more millions of people currently covered through their employer onto the exchanges, will they will find they are paying more for worse coverage and very likely losing access to a lot of the physicians and hospitals they currently prefer to utilize.
We are already seeing this stuff happen which is why I want it stopped.
This only scratches the surface and doesn't touch on the economic harm that will be inflicted through the various tax increases hidden in Obamacare.
Why do you enjoy inflicting harm on millions of people to further your political agenda?
This isn't some abstract discussion in the university faculty lounge anymore. This "reform" is inflicting harm on millions of people and it will only get worse. Why would you support it?
I still don't understand why it will be any more "harmful" nationwide than it was in Massachussetts. Based on their experience, it seems pretty cut and dried that this will be successful and well-liked legislation in the end.
But hey, as a good lib, she's willing to take it for the greater good as long as all of those uninsured get coverage (unfortunately, they are not signing up-but I digress).
The one problem I have with people like our TC friend is they can't come out and admit what is happening: most people are going to pay more under the ACA.
If you still support it, that's your right, but let's just admit the basic facts.
Heck, the winning video for promoting Obamacare is entitled forget about the price tag...
I still don't understand why it will be any more "harmful" nationwide than it was in Massachussetts. Based on their experience, it seems pretty cut and dried that this will be successful and well-liked legislation in the end.
If our old system is so exceptional (which I suppose it is in terms of paying through the nose), why do we spend twice as much per capita as almost every other western country? Seems to me if we adopted the model used by every other western nation - and let's face it, people in these countries have excellent coverage and aren't dying at the hospital doors - we could shave about half the expense out of the healthcare cost equation.
Flyover says we spend $2.7T or so on health care costs per year presently, so I assume if we adopted the Canadian model wholesale, for example, we might spend half that much to cover those presently covered, plus another 50% to increase the level of coverage for those with bad coverage all the while extending coverage to the 40M without. And I point out again, that only 0.5% of Canadians seek treatment in the U.S. every year, primarily because they take sick while traveling here, or because as a much larger country we may offer a particular rare care option their smaller population lacks or does not support. But neither of these reasons have anything to do with rationed care and other such foolishness. Numerous studies have shown this to be true, and I assume a similar number of Americans seek care in Canada, also because they are traveling.
But do think about what our people and our economy could do with an additional $675B to spend in sectors besides health care.
All of this being somewhat beside the point, it does illustrate how wrong it is for critics of the ACA to criticize the bill while offering no alternative save for going back to what we did before. Clearly we can do better. Our peers in the west have demonstrated so.
The fact of the ACA is that it will work well if a wide cross section of the population uses it. It will work poorly if only the sick use it. The time to evaluate its effectiveness will not arrive until several years from now, after the kinks have been worked out of the application process, and after a bigger slice of the population is using the exchanges. Early adopters, as in all situations, will probably have a worse experience than late adopters, but I expect that their challenges and issues will be addressed.
Oh yeah, and MUTGR, what about Versatile's comment above?
And I think Flyover assumes in his cost calculations that the days of the $500k surgeon aren't numbered, among other things.
Last edited by STLviaMSP; 12-05-2013 at 09:57 AM..
I don't need to comment on Massachusetts. I don't know if the Mass plan did in that state what we see happening now across the country as a result of the ACA. What I do know now is that millions of people are being forced out of their current plans and being forced to buy in most cases (from what I can tell), much more expensive plans. And this is just with the individual mandate in the individual health insurance market. THERE IS A REASON THE EMPLOYER MANDATE WAS DELAYED!!!! Millions more will be affected when it kicks in.
Why won't you comment on what is actually happening with the ACA right now?
A non-answer. MA isn't a red herring. It's the best proof of concept we have for the ACA, and it has proven itself to work well. I have no reason to think ACA will play out that differently.
Quote:
Why won't you comment on what is actually happening with the ACA right now?
Because it isn't fully enacted, and an empirical analysis of results will not be possible for several years. I see a very big product rollout made more complicated by its massive scale, and therefore nothing unexpected is happening IMO, thus it isn't comment-worthy. Consequently, I think there is a lot of noise in news reports that focus on the sensational rather than digging deeper to understand whatever trends *might* be discernible, credible, and significant at this early date. After a few years when the complete picture emerges, I'll comment on it. I think short of single-payer, ACA is a good idea.
A non-answer. MA isn't a red herring. It's the best proof of concept we have for the ACA, and it has proven itself to work well. I have no reason to think ACA will play out that differently.
Because it isn't fully enacted, and an empirical analysis of results will not be possible for several years. I see a very big product rollout made more complicated by its massive scale, and therefore nothing unexpected is happening IMO, thus it isn't comment-worthy. Consequently, I think there is a lot of noise in news reports that focus on the sensational rather than digging deeper to understand whatever trends *might* be discernible, credible, and significant at this early date. After a few years when the complete picture emerges, I'll comment on it. I think short of single-payer, ACA is a good idea.
It's not a non-answer. To even begin to compare the MA reform with the ACA, we need to know if MA consumers who had coverage through individual or group plans lost those plans as a result of the MA reform and, if so, whether they were then forced to buy more expensive policies (in many cases double or triple the cost), with high deductibles and out of pocket maximums, often for benefits they don't need or want - such as maternity care for non-child bearing age individuals). This is what is happening RIGHT NOW with the ACA.
Did that also happen in MA? If not, why not - what are the differences between the MA reform in the ACA? I have no doubt that Mitt Romney, given his vast business experience and general acumen, was able to do a better job of reform than Obama, the former community organizer.
If you really want to compare the two you need to start answering some questions.
Last edited by MUTGR; 12-05-2013 at 11:20 AM..
Please register to post and access all features of our very popular forum. It is free and quick. Over $68,000 in prizes has already been given out to active posters on our forum. Additional giveaways are planned.
Detailed information about all U.S. cities, counties, and zip codes on our site: City-data.com.

 Please register to participate in our discussions with 2 million other members - it's free and quick! Some forums can only be seen by registered members. After you create your account, you'll be able to customize options and access all our 15,000 new posts/day with fewer ads.
Please register to participate in our discussions with 2 million other members - it's free and quick! Some forums can only be seen by registered members. After you create your account, you'll be able to customize options and access all our 15,000 new posts/day with fewer ads.