Please register to participate in our discussions with 2 million other members - it's free and quick! Some forums can only be seen by registered members. After you create your account, you'll be able to customize options and access all our 15,000 new posts/day with fewer ads.
The total is not even 5% of the population. So 95% of the American population will NOT get cancer, heart disease, or suffer a heart attack. Stop acting like everyone is going to fall over dead without the ACA because of cancer or heart attack. The argument is ridiculous.
Lol! So, I guess that most people die from shark attacks and meteor strikes?
1. No one can actually pay for their healthcare out of pocket, particularly when it gets serious. So it's stupid to pretend like you're shouldering your full burden when you're not.
2. Therefore, modern healthcare by its very nature functions as a shared communal cost. In other words, it always ends up as "wealth redistribution." For most people, that community is other insurance policyholders (yes, insurance is a fundamentally "socialistic" concept). If it's Medicare, then the community is basically all taxpayers. You need a large pool of people paying in so that the premiums from the healthy can cover the costs of the sick; the diversification of health status among policyholders is what makes it work.
3. Everyone is going to be in the healthcare market at some point, so if you don't have / choose not to get insurance, then others who do have it will have to ultimately pay for you. In other words, you're a financial risk to society and we still end up back at "wealth redistribution." You all say it isn't fair that you're "forced" to have insurance; what about asking how fair it would be to have to pay for others who don't have it, but could?
4. To the extent that you don't think it fair to be stuck with the full burden of someone else's healthcare costs, you should want them to pay something to cover their risk to society (if they can). This is why it fundamentally makes sense to at least charge people a modest fee if they don't want to get into the insurance market.
5. All healthcare is always rationed; it's just a question of which specific entities do the rationing and whether or not the rationing methodologies are rational. It's nothing new. We've been doing it on many criteria here in the USA for a long time now, including: private ability to pay for insurance (just ask the 50 million Americans who are uninsured), employment, pre-existing conditions, comparative effectiveness studies, government eligibility criteria, co-pay / deductible structures...the list goes on and on.
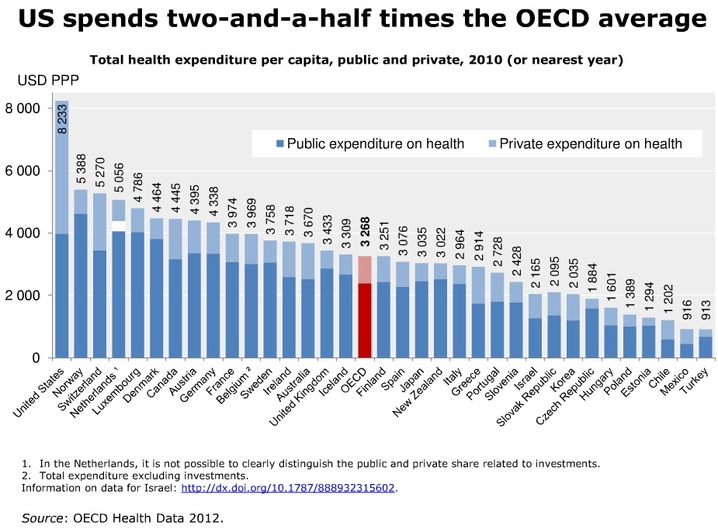
6. While this nation does generally have the best healthcare technology for those lucky enough to be able to access it, statistics show that USA lags other nations in a slew of health outcomes while by far leading in per capita cost. So while Obamacare may not be the way to go, the status quo we've been living with is not cutting it. We can and should demand something better.
So in summary, don't be cowed when people tell you that healthcare will be rationed (duh, it already is) and when they complain about costs being "socialized" or "redistributed" (duh, that's how it has always worked). It's important to understand this when you open your mind to consider what kind system we could ideally have here.
No one pays for their own healthcare because of how our structure is set up in terms of procedure costs and pricing schematics. The very system we've developed to deal with the cost of healthcare costs are remarkably distorted. The coupling of paying for healthcare (treatments, procedures, insurance) SHOULD operate in a similar way to auto insurance, just on a smaller scale. We should be paying for minor procedures, just as they do in countries like Mexico and the price of larger scale treatments should be paid by insurance. Using our insurance for every health expense with excepton to OTC meds is comparable to filing a homeowners claim to paint your walls. Medical billing to insurance companies have distorted the price of treatment so much that people can't afford basic treatments. The root of this issue is wage controls during WW2 which attached insurance to everyones jobs and guess who caused this little conundrum.......The Government. This is a government imposed issue with which the government presumes to hold the keys to the answer.
No. Insurance is a system of individual risk mitigation. It's a communal cost, but only because we all pay our premium. This isn't even remotely socialistic. Medicare and Medicaid are different, but individual insurance is not.
This point is often touted by the left as a justification for a single-payer system, however the costs of paying for treatment for the random people that slide into an ER for a cold, or show up in the throughs of cardiac arrest aren't nearly as common as you would be lead to believe. All businesses are required to eat costs to be in the marketplace. Literally, no business is immune from this. If procedures themselves were less expensive and health insurance were affordable (as they would be in treated to a true market mechanism) the true number of uninsured would naturally be lower.
Again...this is a symptom of a government instigated problem. The whole "cost-sharing" thing is because the costs are so high. If the market were allowed to work on treatment costs as opposed to enlarging the problem, we wouldn't have nearly the issue that we have in terms of people lacking the ability to afford the treatment. As it stands, the regulatory structure has effectively killed any market mechanism for healthcare. Thank god that my eye insurance doesn't cover contact lenses. Because of this, they have gone from very expensive to downright cheap now. Had the government mandated that insurers in my state cover them...they would still be insanely overpriced.
.....m'kay.
We have the best healthcare and healthcare technology in the world. That is why foreign leaders come here for treatment. The arbitrary figures thrown out by the WHO have been disputed for years and years. The issue with cost per capita...see the link below.
Totally devoid of any common sense....no surprise there.
Let's see....you rail against an oil cartel, namely OPEC, because you falsely believe that OPEC illegally colludes to illegally fix the price of oil.....when in fact and reality OPEC oil prices per barrel are lower than non-OPEC oil producing States...uh, like Canada.
No idea what you are talking about...I haven't said anything about OPEC, and it bears no relation to this topic.
Yes, healthcare providers put a big markup on services. I never claimed they didn't. What does that have to do with the price of tea in China? The point is that Americans still can't typically afford out of pocket healthcare, whether marked up or not. This is not a controversial statement.
Besides, I thought you were a conservative. Now you don't like that these entities with disproportionate power can ration your care and manage their financial statements through pricing power? Sounds like you're becoming a socialist...haha.
Quote:
Originally Posted by Mircea
So...according to you.....charging $41,000 for a surgery that actually costs $13,000 is just pure common sense.
Saying I said things which I never even remotely uttered makes you look unhinged and hurts your credibility.
Quote:
Originally Posted by Mircea
That is a logical fallacy known as a non-sequitur.
No, it is NOT. A non-sequitur is when the conclusion does not follow from the facts. In what I say, the fact of how health insurance works clearly concludes in the fact that it functions solely to pool together expenses and revenues so that expenses that could not be borne by the individual are managed through a diversified pool of policyholders. This is how insurance works; it's not controversial.
Quote:
Originally Posted by Mircea
That is contrary to the Principles of Actuarial Science.....
Nothing you posted showed anything contrary to my statement.
Quote:
Originally Posted by Mircea
Suffice to say that nobody pays for the "uninsured."
....and read the very informative information about losses.
You're dribbling nonsense out of your mouth again. No one pays directly for the uninsured, but of course you pay indirectly for them. What do you think, the hospital is just going to keep incurring losses? They'll jack up the prices on others over time. I'm not saying it's the main driver of cost increases (it's not), but it's stupid to think that powerful healthcare-providing entities will not extract losses they incur on one segment by raising prices on the other segments over time.
Quote:
Originally Posted by Mircea
Rationing is extremely well-defined in the medical literature and professional journals, and the definitions are posted all over C-D....
Sigh... can you maybe buy a clue? Or phone in?
It doesn't take a genius to understand that every nation on earth must ration their healthcare in some way. It's related to something called "the principles of economics."
Rationing in the United States is not a top-down, centralized policy imposed by the government. In the absence of a universal health program, rationing occurs in both the public and private health care sectors. It is practiced by government agencies, private health insurance companies, hospitals, and providers, in ways both official and unofficial, intended and unintended, visible and invisible. The American way of rationing is a complex, fragmented, and often contradictory blend of policies and practices, unique to the United States.
Quote:
Originally Posted by Mircea
Let's see what the United States Center for Disease Control has to say about the so-called "infant mortality rate" in the US....
Three studies by people smarter than you showing where USA lags:
The exclusion of any high-risk infants from the denominator or numerator in reported IMRs can be problematic for comparisons. Many countries, including the United States, Sweden and Germany, count an infant exhibiting any sign of life as alive, no matter the month of gestation or the size, but according to United States some other countries differ in these practices. All of the countries named adopted the WHO definitions in the late 1980s or early 1990s,[33] which are used throughout the European Union.[34] However, in 2009, the US CDC issued a report that stated that the American rates of infant mortality were affected by the United States' high rates of premature babies compared to European countries. It also outlined the differences in reporting requirements between the United States and Europe, noting that France, the Czech Republic, Ireland, the Netherlands, and Poland do not report all live births of babies under 500 g and/or 22 weeks of gestation.[35][36][37] The report concluded, however, that the differences in reporting are unlikely to be the primary explanation for the United States’ relatively low international ranking
Quote:
Originally Posted by Mircea
...if Euro-States are spending more money on Social Services related to health care than the US, then how is health care in Euro-States cheaper or more affordable?
This is a quintessential example of how you lie. You mix two things together that are unrelated.
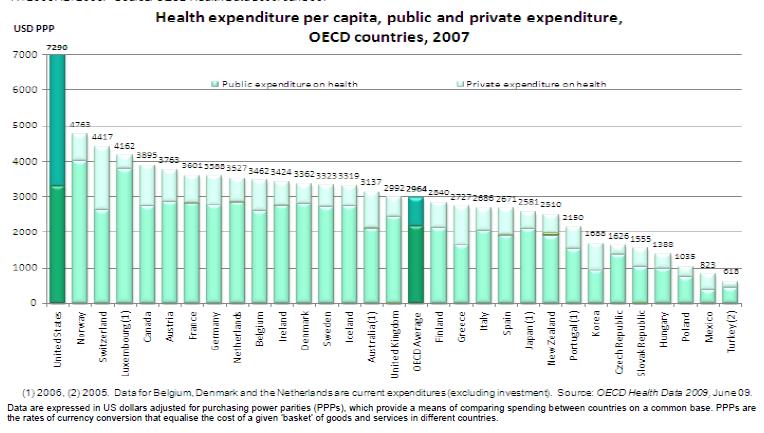
You mix together healthcare expenditures and social expenditures, knowing that EU spends more on other aspects of its social network than the USA does that that it will bias the result in your favor. It's apples and oranges, and your own damn graph shows how you're lying.
LOOK AT THE BLUE BAR IN YOUR OWN GRAPH. It's far and away the highest for the USA. And here are some more:
The gap between US healthcare expenditures vs. outcomes has been well-documented from many perspectives.
Quote:
Originally Posted by Mircea
How could someone possibly have an open mind when you hide the Truth from them?
Common sensibly....
Mircea
Psst...
Your shtick is getting old, and it's not working....
Why not a system where in Canada no-one rations it. The government stays out of medical decisions completely; what treatment you get etc. is determined by your doctor. The only role the government plays is to pay the bills - nothing else.
You don't need to go full on socialised healthcare, a single payer option would be a better option that what you have now.
Healthcare everywhere is rationed unless one can pay cash at the point of service. Canada is no exception.
Drug manufacturers know to the pill which MDs prescribe their products. Drug manufacturers reward their top producing MDs with stock options, fellowships and compensated board/advisory panel appointments. This is not to say that all MDs are eligible or even want to be. This sort of stuff does not happen in the rest of the developed world.
The rest of the developed world maintains objective panels of MDs who compare and contrast the cost and effectiveness of medications. If brand A and B achieve the same outcome, the least costly medication should be used. This is an example of the strategies employed elsewhere to reduce the cost of healthcare.
This was in the initial version of the ACA, the one Republicans claimed they did not have an opportunity to read. Yet, they were quick to pounce on the concept of comparative/effectiveness panels as death panels and in doing so, continued to protect the Big Pharma lobbies. It was subsequently withdrawn.
What factual information within ACA leads you to believe that government will make healthcare decisions for you?
The GOVERNMENT rations it by providing limited facilities, resources, technology, and personnel. The "cost" is contained by simply not having enough resources to meet everyone's needs. That is how EVERY single payer system does it. They choose whom to let die and whom to attempt to help. And the subject has no influence on the decision.
Are there reports from the rest of the developed world that the masses are dying in the streets because their governments will not treat them?
ACA is not universal healthcare.
The co-pay is one of the most common tactics used to ration healthcare in the developed world.
No two nations with universal healthcare have the same laws/systems. Strategies used to control costs vary nation to nation and include but are not limited to:
Government owned /operated hospitals, or
Physician-owned hospitals, or
No corporate owned hospitals, and
Preventative Medicine, and
Negotiating the price of prescription medications and devices, and
Limiting the compensation of Sr. hospital administers, and
Not spending $ on advertising, and
Compelling a wait time for elective procedures, and
Maintaining objective MD comprised Comparative-Effectiveness Panels to evaluate medications and protocols, and
A culture that is not litigation crazed, and
in some cases more MDs per capita with education paid for by tax payers
There have been some problems in the healthcare system, that doesn't make the ACA good. Yes insurance companies deny claims, but Medicare denies a higher percentage than the private insurance companies.
The small potato insurers who cannot compete on a level playing field did not negotiate PPO arrangements.
The uninsured/underinsured and those paying cash pay the most.
Healthcare costs in the U.S. are less in those areas where healthcare is highly competitive. The opposite is true in those areas, often rural, where competition is limited.
But, think of cost pooling like this: You walk into your favorite restaurant, and there's a sign that says "cheques will be pooled tonight". Which means that everyone's going to have their bill pooled with everyone else and you'll only pay the average.
Who is going to be frugal? Why would they?
All insurance and consumer prices are based on the pooling (mutualization) of risks.
Do most people total their cars because they carry insurance?
Do most people burn their homes down because they are insured?
Do most people kill themselves so that the beneficiary of their life insurance policy gets a pay day?
Do most businesses behave in a reckless manner and invite lawsuits because they carry D&O and liability insurance?
In my neck of the woods, a 55 year old will pay 35-60% more for health insurance dependent upon the plan and insurer they choose.
The cost of doing business is factored into the price we pay for everything. The cost of shop lifting/return scams, bad debt and faked liability is a factor of the price of all goods.
Your shtick is getting old, and it's not working....
On infant mortality statistics, I part company with some of my fellow "liberals". I do not believe comparative statistics, and I will quote some previous posts of mine that show why. In particular, first day mortality is hard to compare when some countries don't count an infant as a live birth unless it lives more than 24 hrs!
Quote:
Originally Posted by Katiana
Actually, on this one issue, I disagree, and so do the stats. Here is a post I made last night about this issue.
(Post is below)
Another quote from this article that concerns Canada:
** Neonatal deaths under 500 g, as a proportion of all neonatal deaths, also ranged from less than 1% in countries such as Luxembourg and Malta to 29.6% in Canada and 31.1% in the United States. **
Canada, like the US, uses the WHO definition of a live birth.
Here's another table. Canada's rate is lower, but "WAY lower" is an exaggeration, especially since both rates are low to begin with.
There is a table in here that shows that at most birthrates, there is not much difference at all. In some cases the US' is lower, in some cases, Canada's. Please note I am not saying I agree with everything in this article. Health Care System Grudge Match: Canada vs. U.S. « Healthcare Economist
**The World Health Organization’s International Statistical Classification of Diseases and Related Health Problems has long defined a live birth as any product of conception that shows signs of life at birth, with no consideration for birthweight or gestational age criteria.13 Although this definition remains unchallenged, countries have widely varying regulations for registration of birth that range from definition based to pragmatic. For instance, birth registration is required for all live births that satisfy the WHO’s definition of live birth in Canada, England and Wales, and the United States,15 25 whereas countries such as the Czech Republic, France, and the Netherlands specify limits based on some combination of gestational age (for example, at least 22 weeks), birth weight (for example, at least 500 g), or survival (for example, any live birth irrespective of birth weight that survives the first 24 hours after birth) (web appendix table C).18 26 27 Procedural differences due to longstanding traditions, social attitudes, and local incentives (including financial remuneration of healthcare providers) also probably dictate whether an infant at the borderline of viability is registered.
Conclusions International differences in reported rates of extremely low birthweight and very early gestation births probably reflect variations in registration of births and compromise the validity of international rankings of perinatal and infant mortality.**
The cost of healthcare will continue to INCREASE as the spending (decision) is DISTANCED from the healthcare transaction.....
(remember, ECON 101, spending someone else's money? I may as well get all I can..... "it's paid for already")
In the beginning, it was between patient - doctor
Then, between employeR - HMO
Now, ACA.... moves it farther away.
The only 'saving grave' may be the $5,000 deductibles...... (typo/pun intended )
And yet, the rest of the developed world spends substantially less for healthcare than those in the U.S. Please explain.
Last I checked, dead people were not piling up in the streets of Germany and Switzerland due to lack of, or shoddy care.
Please register to post and access all features of our very popular forum. It is free and quick. Over $68,000 in prizes has already been given out to active posters on our forum. Additional giveaways are planned.
Detailed information about all U.S. cities, counties, and zip codes on our site: City-data.com.

 Please register to participate in our discussions with 2 million other members - it's free and quick! Some forums can only be seen by registered members. After you create your account, you'll be able to customize options and access all our 15,000 new posts/day with fewer ads.
Please register to participate in our discussions with 2 million other members - it's free and quick! Some forums can only be seen by registered members. After you create your account, you'll be able to customize options and access all our 15,000 new posts/day with fewer ads.




 )
)
