Please register to participate in our discussions with 2 million other members - it's free and quick! Some forums can only be seen by registered members. After you create your account, you'll be able to customize options and access all our 15,000 new posts/day with fewer ads.
Its always the same pattern, bombardment with TV ads for the new drug and a few years later ads from lawyers for all the people harmed by the drug.
I don't know. I never even tried and refused anything besides insulin even though I am a so called LADA
"Type 1.5 diabetes is a form of “double” diabetes because people with this condition show both the autoimmune destruction of beta cells of type 1 diabetes and the insulin resistance characteristic of type 2 diabetes."
All I know is insulin works. Get by on Lantus.
Last edited by Oldhag1; 12-18-2022 at 04:55 AM..
Reason: Moved to own thread
Since it requires injection anyway, why not just use Insulin instead of Ozempic or the other new drugs like it?
Quote:
Originally Posted by BarefootDiabetic
If you have to inject anyway why would anyone inject "Ozempic" or anything "newly approved" instead of insulin?
.
Good point (can't rep you again yet)
You're right on the practical level. The theory is that the newer drugs "get right to the point" where as insulin is a "shot gun approach" that can be counter productive when started too early in T2 DM.
Early T2 is generally characterized by elevated insulin levels. Insulin stimulates lipogenesis (storing fat in fat cells.)...I like to think of fat cells as prisons and insulin as the guards on the prison walls-- the bigger the prison, the more guards you need and hiring more guards also means increasing the size of the prison-- a viscious, counter productive cycle.
That's why so many docs who only calculate "success" as achieving lower BS/HbA1c levels start insulin too early, then have to periodically increase insulin dosage to maintain the "good results. ...More insulin means more fat--> More fat means you need more insulin...and you keep chasing your own tail.
You're right on the practical level. The theory is that the newer drugs "get right to the point" where as insulin is a "shot gun approach" that can be counter productive when started too early in T2 DM.
Early T2 is generally characterized by elevated insulin levels. Insulin stimulates lipogenesis (storing fat in fat cells.)...I like to think of fat cells as prisons and insulin as the guards on the prison walls-- the bigger the prison, the more guards you need and hiring more guards also means increasing the size of the prison-- a viscious, counter productive cycle.
That's why so many docs who only calculate "success" as achieving lower BS/HbA1c levels start insulin too early, then have to periodically increase insulin dosage to maintain the "good results. ...More insulin means more fat--> More fat means you need more insulin...and you keep chasing your own tail.
Guido since you are knowledgeable about diabetes, I have a question pertaining to what you just said. I am 73 and newly diagnosed; however have been running higher #'s than normal for many years. I was hospitalized recently from an accident which drove my glucose through the roof; so they gave me a lot of insulin to bring it down for me to have my surgery, which I did (knee surgery)
I am now seeing my regular PCP who has reduced my insulin dramatically; however keeping a watch on it. From my standpoint, at my age I have no interest in trying to drive my #'s too low. I am now injecting Lantus (20 units) once per day, my #s range from 100 - 135 on average, but higher later in the day. It doesn't seem to matter what or how much I eat or even if I don't eat; however in the a.m. it rises higher if I get up too late (dawn phenomenon). Based on this info, what advice would you have for me or my doctor?
If you have to inject anyway why would anyone inject "Ozempic" or anything "newly approved" instead of insulin?
Its always the same pattern, bombardment with TV ads for the new drug and a few years later ads from lawyers for all the people harmed by the drug.
I don't know. I never even tried and refused anything besides insulin even though I am a so called LADA
"Type 1.5 diabetes is a form of “double” diabetes because people with this condition show both the autoimmune destruction of beta cells of type 1 diabetes and the insulin resistance characteristic of type 2 diabetes."
All I know is insulin works. Get by on Lantus.
Injecting once a week is vastly preferable to injecting insulin multiple times a day. Plus, for me it controls the extreme sugar level swings I experienced prior to using this family of drug.
This drug is not appropriate for type I diabetics, it is not designed to address the problems of those whose beta cells no longer function. I would think it could still be used for insulin resistance in LADA but I don’t think they have done the testing on it.
__________________
When I post in bold red that is moderator action and, per the TOS, can only be discussed through Direct Message.
Injecting once a week is vastly preferable to injecting insulin multiple times a day. Plus, for me it controls the extreme sugar level swings I experienced prior to using this family of drug.
This drug is not appropriate for type I diabetics, it is not designed to address the problems of those whose beta cells no longer function. I would think it could still be used for insulin resistance in LADA but I don’t think they have done the testing on it.
Exactly.
First point is that insulin is still the standard (and a life saver) for Type I diabetics.
However, for Type 2...well...medical knowledge and advancements have given us more (and better) options.
For many Type 2, insulin helps keep the blood glucose lower, but also has a secondary effect of causing weight gain. Ozempic (and others like it) do not, and in fact can help to lose weight, thereby having a higher net benefit to many Type 2 diabetics.
As our knowledge increases, our treatment gets better. It makes sense to take advantage of it.
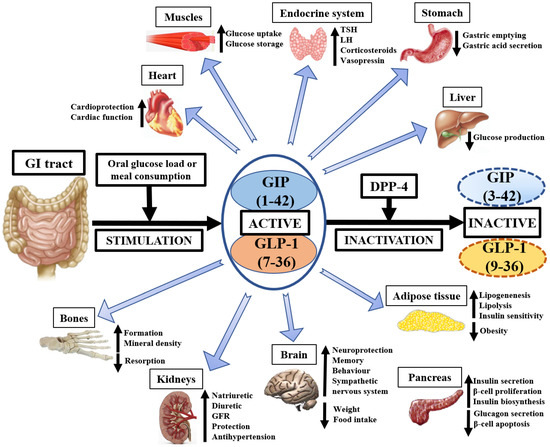
GLP agonist drugs do more than just manage insulin and glucose levels. They work on multiple organs and systems, from gut to brain to pancreas to the heart, to the thyroid, just to name some. GLP receptors are found in many organs, and that's what makes this class of drugs so powerful. Inflammation is reduced in the body, satiety is activated, gastric emptying is slowed down, etc. Insulin doesn't do those things.
The newest GLP-1 and GIP peptides work on the following:
Guido since you are knowledgeable about diabetes, I have a question pertaining to what you just said. I am 73 and newly diagnosed; however have been running higher #'s than normal for many years. I was hospitalized recently from an accident which drove my glucose through the roof; so they gave me a lot of insulin to bring it down for me to have my surgery, which I did (knee surgery)
I am now seeing my regular PCP who has reduced my insulin dramatically; however keeping a watch on it. From my standpoint, at my age I have no interest in trying to drive my #'s too low. I am now injecting Lantus (20 units) once per day, my #s range from 100 - 135 on average, but higher later in the day. It doesn't seem to matter what or how much I eat or even if I don't eat; however in the a.m. it rises higher if I get up too late (dawn phenomenon). Based on this info, what advice would you have for me or my doctor?
Not knowing the details of your case, I can only talk in generalities--
An illness or injury puts you under physiological stress-- more adrenalin, cortisone, etc being secreted and BS levels tend to go up. Hosp pts often need insulin to get things under cntrol and can usually be stopped after the extra stresses subside....
Lantus is given to serve as "background insulin" so there's always some in your system, as opposed to shorter acitng insulin given multiple times during the day to cover new glucose coming into your system as you eat meals.
The natural course of T2 DM is to secrete insulin in excessive quantities when you're young, and if diet rstictions are not well followed, the pancres will eventually poop itself out and the insulin levesl fall too low. Teh classic exoample is the over-weight diabetic who takes oral meds but is only border-line cointrolled, and then more or less suddenly starts losing a lot of weight and BSs start going up. The pt has become insuliopenic and needs to be put on insulin.
Many studies show that older pts, particularly those hospitalized, do better (fewer complications) if measures to control BS are more relaxed. Like hi BP, hi BS is important in the long run rather than minute to minute control...We're both 73...We just don't have a long run left to worry about.
Guido since you are knowledgeable about diabetes, I have a question pertaining to what you just said. I am 73 and newly diagnosed; however have been running higher #'s than normal for many years. I was hospitalized recently from an accident which drove my glucose through the roof; so they gave me a lot of insulin to bring it down for me to have my surgery, which I did (knee surgery)
I am now seeing my regular PCP who has reduced my insulin dramatically; however keeping a watch on it. From my standpoint, at my age I have no interest in trying to drive my #'s too low. I am now injecting Lantus (20 units) once per day, my #s range from 100 - 135 on average, but higher later in the day. It doesn't seem to matter what or how much I eat or even if I don't eat; however in the a.m. it rises higher if I get up too late (dawn phenomenon). Based on this info, what advice would you have for me or my doctor?
Steroid pills will usually raise your blood sugar 4 to 8 hours after you take them. For example, if you take a steroid like prednisone in the morning, your blood sugar will likely increase later in the day, most commonly after lunch and before supper. Intravenous (IV) steroids will raise your blood sugars sooner.
That was just paste but my diabetic neighbor warned me about prednisone , he is 76.
GLP agonist drugs do more than just manage insulin and glucose levels. They work on multiple organs and systems, from gut to brain to pancreas to the heart, to the thyroid, just to name some. GLP receptors are found in many organs, and that's what makes this class of drugs so powerful. Inflammation is reduced in the body, satiety is activated, gastric emptying is slowed down, etc. Insulin doesn't do those things.
The newest GLP-1 and GIP peptides work on the following:
Good I just want my blood sugar down, I have an insulin deficiency my body does not lack ozempic, your graphic shows every body system confused by a foreign man made substance and going up down and sideways. Memory and behavior too? My gosh!
Like playing a piano with oven mitts that Ozempic, you cant hit one key without hitting a bunch of others!
Good I just want my blood sugar down, I have an insulin deficiency my body does not lack ozempic, your graphic shows every body system confused by a foreign man made substance and going up down and sideways. Memory and behavior too? My gosh!
Like playing a piano with oven mitts that Ozempic, you cant hit one key without hitting a bunch of others!
Good point...BS control is very complex, and changing one thing always incites a reciprocal change in all the other factors.
Compare using insulin to warming a cold house-- The house may be cold for many reasons-- bad furnace, clogged air ducts, bad insulation etc. You coould take pains to find the real cause and just fix that, or you could just build a bigger fire in the middle of the room and forget it. You'd certainly get warmer, but maybe burn the house down too, but maybe not...What you do depends on the individual circumstance. Risk vs benefit.
For pts doing well, no need to change. For those with less than acceptable results, may as well try somethiing different.
Please register to post and access all features of our very popular forum. It is free and quick. Over $68,000 in prizes has already been given out to active posters on our forum. Additional giveaways are planned.
Detailed information about all U.S. cities, counties, and zip codes on our site: City-data.com.

 Please register to participate in our discussions with 2 million other members - it's free and quick! Some forums can only be seen by registered members. After you create your account, you'll be able to customize options and access all our 15,000 new posts/day with fewer ads.
Please register to participate in our discussions with 2 million other members - it's free and quick! Some forums can only be seen by registered members. After you create your account, you'll be able to customize options and access all our 15,000 new posts/day with fewer ads.